Who Should Get a Bone Density Test and When to Start Monitoring
Also known as osteoporosis screening or a bone mineral density (BMD) test, this guide helps you understand when to schedule a bone density test and what your options are. After learning how bone loss develops and how newer technology is making monitoring easier the next logical question is:
Do I actually need to get my bone health checked right now?
For many people, the answer comes down to timing. And in bone health, timing matters more than most realize.
The Traditional Guidelines (And Their Limitations)
If you’ve searched for terms like “when should I get a bone density test” or “osteoporosis screening age”, these are the recommendations you’ll typically find. Standard recommendations suggest:
- Women begin screening at age 65
- Men begin screening at age 70
- Earlier testing for those with risk factors
These guidelines are helpful but they are often reactive rather than preventative. By the time many patients reach these milestones:
- Bone loss may already be significant
- Osteopenia may have progressed to osteoporosis
- Opportunities for early intervention may have been missed
The Limitations of Traditional Bone Density Testing
Dual-energy X-ray absorptiometry (DEXA) has long been the standard for measuring bone density. While it remains a valuable diagnostic tool, it was not designed for proactive, ongoing monitoring. Common limitations include:
- Exposure to low-dose radiation, limiting how often testing is performed
- Infrequent testing intervals, often one or more years apart
- Focus primarily on bone density, not overall bone quality
- Limited ability to detect subtle changes early
For many patients, this means bone health is only evaluated periodically rather than continuously tracked over time.
Why Earlier Testing Is Often More Valuable
Many patients searching for a bone health test or bone density test near me are surprised to learn that earlier screening can provide more actionable insight. Bone health doesn’t suddenly change at 65 it evolves gradually over decades. Peak bone mass is typically reached around age 30, after which bone density begins to decline. That means for many adults:
- Bone loss may already be underway in their 30s or 40s
- Changes may occur long before symptoms appear
- Waiting for “recommended age” may delay early detection
Establishing a baseline earlier provides a critical advantage. For many patients, this means bone loss may already be occurring before they ever consider testing.
Who Should Consider a Bone Density Test Sooner?
If you’re wondering “do I need a bone density test”, these risk factors can help guide that decision. You may benefit from earlier screening if you:
- Are over age 30 and want a baseline
- Have a family history of osteoporosis or fractures
- Have experienced a previous fracture from a minor fall
- Have low body weight or nutritional deficiencies
- Are postmenopausal or experiencing hormonal changes
- Take medications that impact bone density (e.g., steroids)
- Have chronic conditions affecting bone health
Even without symptoms, these factors can increase your risk of bone loss. Many patients are surprised to learn they qualify for earlier screening based on these factors alone.
What About Symptoms? Should You Wait for Them?
Patients often look for osteoporosis symptoms before seeking testing—but waiting for symptoms can delay early detection. In most cases, no.
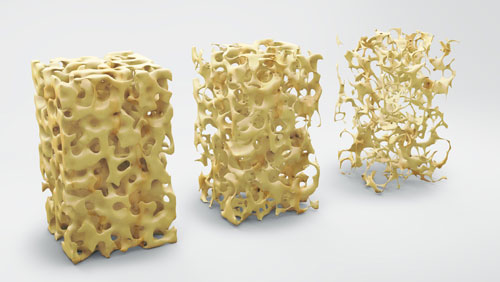
Osteoporosis is often called a “silent disease” because it develops without noticeable symptoms until a fracture occurs. By the time symptoms like height loss, back pain, postural changes appear, bone loss is often already advanced.
This is why proactive testing not reactive care is key.
The Role of Baseline Testing
A baseline bone mineral density test helps establish where your bone health stands today and supports more accurate long-term monitoring. A baseline bone density assessment provides:
- A clear starting point for your bone health
- Insight into whether bone loss has already begun
- A reference for tracking changes over time
At CSOG, this baseline becomes the foundation for a personalized care plan designed to:
- Strengthen bone health
- Reduce fracture risk
- Prevent progression before it becomes severe
How Often Should You Be Tested?
If you’ve searched “how often should you get a bone density test”, the answer depends on your individual risk and the type of testing used.
Testing frequency depends on:
- Your age
- Risk level
- Previous results
With traditional methods, testing is often spaced years apart. However, newer approaches, like Echolight REMS (often compared in searches like “DEXA scan vs ultrasound bone density test”), allow for:
- More frequent monitoring
- Earlier detection of subtle changes
- Better tracking of progress over time
This supports a more continuous, proactive approach to care. With quick, radiation-free options like Echolight, getting a baseline is easier and more accessible than many patients expect.
What to Expect at CSOG
If you’re looking for a bone density test near you, CSOG offers advanced, in-clinic screening with immediate results.
At Colorado Springs Orthopaedic Group, the process is designed to be simple, efficient, and personalized.
- A quick, noninvasive scan provides insight into bone density and fracture risk
- Results are used to guide a customized care plan
- Follow-up appointments focus on monitoring progress and adjusting your plan
This approach ensures that care is not only diagnostic but ongoing and preventative.
So When Should You Start?
If you’ve been asking “when should I get tested for osteoporosis”, the answer is often sooner than expected based on your individual risk profile. If you’re asking the question, that’s often your answer. For many patients, the right time to start monitoring bone health is:
- Earlier than expected
- Before symptoms appear
- Before significant bone loss occurs
If you’re unsure whether it’s time to check your bone health, a baseline assessment can provide clarity and direction. If you’re over 30 or have any risk factors, establishing a baseline now can help you take control of your bone health early before changes progress.
At CSOG, a quick, radiation-free scan offers immediate insight so you can understand where you stand today and take the right next step for your long-term health.