Quadriceps-Sparing Total Knee Replacement: What to Know
Quadriceps-sparing total knee replacement is a contemporary approach to knee arthroplasty that preserves the quadriceps tendon and limits trauma to surrounding soft tissues. By avoiding a large incision through the quadriceps tendon, this technique is intended to support early mobility, reduced postoperative pain, and help patients resume daily activities sooner. Below, learn how the procedure works, how it compares with traditional methods, the Jiffy Knee approach, and who may be a good candidate. For patients searching for the latest in knee replacement surgery, the quad sparing total knee replacement technique is a thoughtful, evidence-informed choice that our team carefully considers for each individual.
What Is Quadriceps-Sparing Total Knee Replacement?
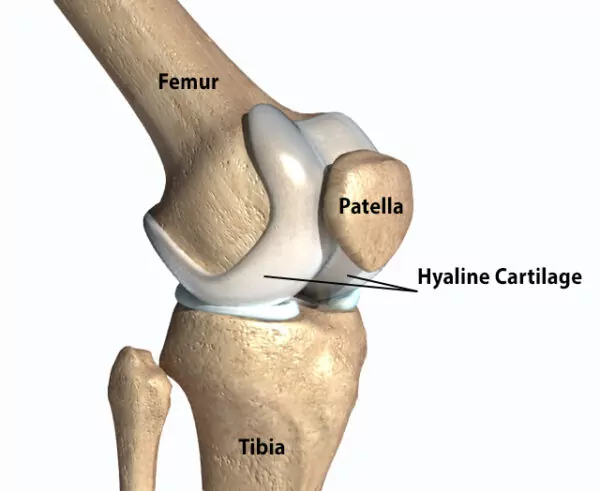
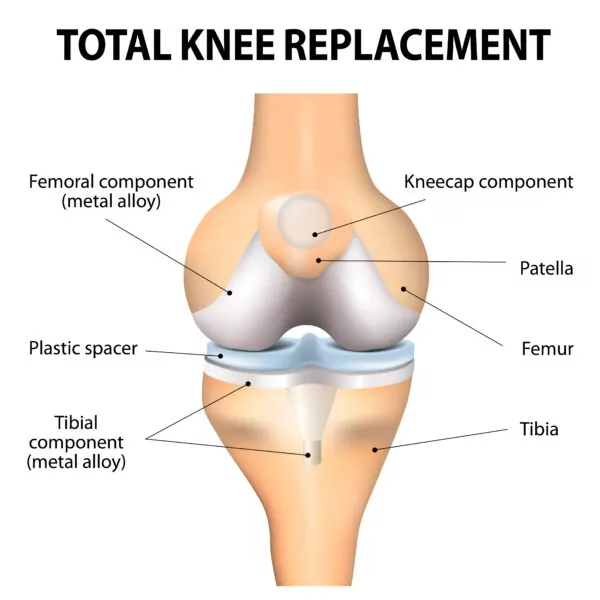
This procedure replaces damaged joint surfaces in the knee while maintaining the integrity of the quadriceps tendon and extensor mechanism. Surgeons work around the tendon rather than through it, navigating between natural tissue planes to access the joint and accurately position implants. In plain terms, if you have wondered, “are muscles cut during knee replacement surgery?” the goal with a quad sparing knee replacement is to avoid cutting the quadriceps tendon and minimize disruption of surrounding muscle fibers whenever safely possible.
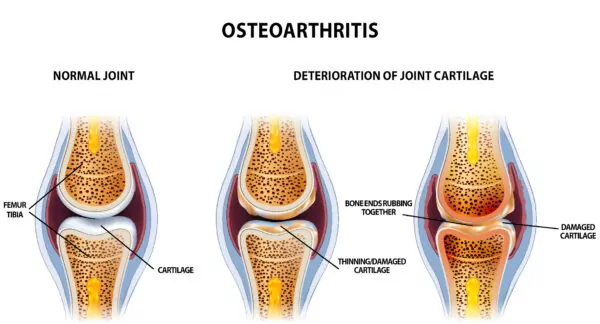
The technique evolved from approaches developed in the early 1990s.1 As specialized instruments and imaging guidance improved, surgeons refined methods to avoid splitting the quadriceps tendon without compromising implant alignment or stability. It is commonly used to treat severe osteoarthritis and other advanced degenerative conditions that cause pain, stiffness, and loss of function when non-surgical measures are no longer effective. Among the types of knee replacement available today, quad sparing total knee replacement is considered part of the latest in knee replacement surgery, focused on soft tissue preservation and early function.2
Benefits of a Quadriceps-Sparing Approach
- Faster early recovery: Preserving the quadriceps tendon can facilitate earlier straight-leg raises, walking, and stair climbing.3
- Less muscle disruption: Protecting the extensor mechanism may help maintain strength and knee control, supporting a more efficient rehabilitation process and a quicker return to a normal gait. Patients often ask, “are tendons and ligaments cut during knee replacement?” With a quadriceps-sparing technique, the aim is to protect the entire quadriceps mechanism to reduce postop dysfunction.4
- Reduced early pain and swelling: Limiting soft tissue trauma often improves comfort in the first weeks after surgery and may reduce the need for inpatient rehabilitation.3,5
All surgical procedures carry risks such as infection, blood clots, stiffness, implant loosening, and anesthesia-related issues. Careful surgical technique, multimodal pain control, and early mobilization help mitigate many of these risks. Long-term outcomes with quadriceps-sparing techniques are comparable to traditional approaches when performed by experienced surgeons. If you have concerns about “how are muscles reattached after knee replacement,” rest assured that when muscle or tendon detachment is required in other approaches, surgeons use robust suture techniques to reattach and protect healing; with quad sparing knee replacement, the intention is to avoid muscle separation in the first place.
How It Differs From Traditional Knee Replacement
Surgical exposure: Traditional total knee replacement often uses a midline incision with a split in the quadriceps tendon separating the vastus medialis from remaining three quadriceps muscles to access the joint. Quadriceps-sparing techniques use a muscle sparing approach to avoid cutting the tendon, preserving the extensor mechanism. This directly addresses concerns such as “are muscles cut during knee replacement surgery,” as the quad sparing total knee replacement approach is designed to minimize that need.
Rehabilitation and function: Because the tendon remains intact, patients can typically begin active knee extension earlier. Many experience less early pain and greater confidence with movement, which can translate into smoother physical therapy sessions and faster achievement of mobility milestones.2,3,4,5
Outcomes: Early recovery measures—pain, range of motion, and function—have been shown to be improved with quadriceps-sparing methods. Long-term implant performance and overall function are similar to traditional techniques when alignment and soft tissue balancing are precise around 1 year postoperatively. For those asking “how are muscles reattached after knee replacement,” traditional methods may require tendon repair; quadriceps-sparing methods are designed to avoid that step while maintaining accuracy.
Quadriceps-Sparing vs. Jiffy Knee
Jiffy Knee is a branded, muscle-sparing total knee replacement approach that emphasizes limited disruption to the quadriceps and surrounding soft tissues. Both quadriceps-sparing and Jiffy Knee aim to reduce early pain and speed recovery by protecting the extensor mechanism through the same medial subvastus approach to the joint. Patients comparing a quad sparing knee replacement to a jiffy knee replacement will find overlapping principles focused on soft tissue preservation.
| Feature | Quadriceps-Sparing TKA | Jiffy Knee |
|---|---|---|
CORE PRINCIPLE | Avoids incising the quadriceps tendon; uses tissue planes to access the joint | Branded muscle-sparing technique with similar tendon-preserving goals |
INCISION AND EXPOSURE | Medial subvastus muscle sparing approach; standard instruments or specialized tools | Proprietary instruments and protocols may be used through the same medial approach and a more medial incision |
RECOVERY FOCUS | Earlier straight-leg raises, walking, and confidence with movement | Marketed for rapid recovery with early function and reduced pain |
OUTCOMES | Early advantages with comparable long-term results to traditional TKA | Similar expectations: outcomes depend on surgeon expertise and implant alignment |
In practice, the similarities are greater than the differences. Both rely on the concept of a muscle sparing approach to the knee, careful soft tissue handling, and precise implant positioning. The best choice is often the technique your surgeon performs most frequently and effectively, tailored to your knee anatomy and goals. When considering what technique might suit your knee replacement best, our guidance remains individualized and focused on safety and function.
Who Is a Good Candidate?
- Advanced knee osteoarthritis or other degenerative conditions causing significant pain and mobility limitations despite non-surgical care
- Favorable soft tissue quality and alignment that allow adequate exposure without cutting the quadriceps tendon
- Realistic expectations and willingness to participate in a structured rehabilitation program
Both younger, active adults and older patients can be candidates. Suitability depends more on joint damage, bone quality, and overall medical fitness than age alone. Active individuals may appreciate faster early recovery, while older adults may benefit from reduced pain and earlier independence. Not every knee is appropriate for a quadriceps-sparing or jiffy knee replacement approach; some patterns of deformity or prior surgery may necessitate alternative types of approach to knee replacement.
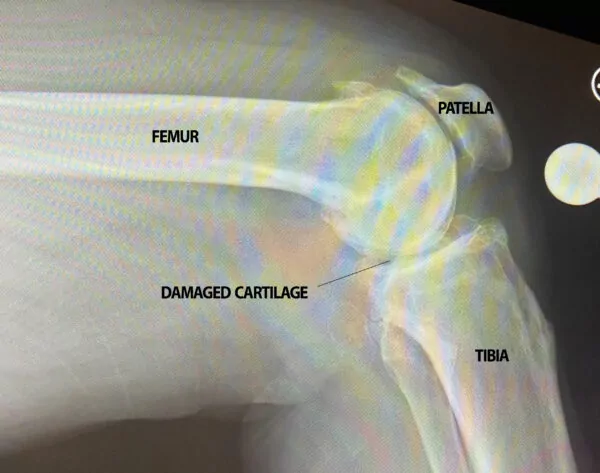
The evaluation typically includes a full medical history, physical examination, weight-bearing X-rays, and sometimes advanced imaging. If you have questions like “are tendons and ligaments cut during knee replacement,” we will explain how quadriceps-sparing techniques aim to preserve these structures while still achieving proper alignment and stability.
What to Expect
Most patients begin walking with assistance the day of their surgery and start physical therapy focused on range of motion, swelling control, and progressive strengthening within a week. Many can perform basic daily activities within a few weeks, though full recovery varies based on individual factors and adherence to rehabilitation. Your care team will provide guidance on wound care, medications, activity progression, and long-term joint protection. As part of the latest in knee replacement surgery, our protocols emphasize comfort, safety, and steady progress.
If you are considering knee replacement and want to know whether a quadriceps-sparing total knee replacement is right for you, schedule a consultation with Dr. D. Alex Forrester, who specializes in quadriceps-sparing knee replacements. A personalized assessment can help determine the safest technique that aligns with your anatomy, goals, and lifestyle—whether that is a quad sparing total knee replacement or another evidence-based option among the types of knee replacement we offer.

References:
- Hofmann, A.A. ∙ Plaster, R.L. ∙ Murdock, L.E. Subvastus (southern) approach for primary total knee arthroplasty. Clin Orthop Relat Res.1991; 70-77
- Stubnya B, Kocsis K, Váncsa S. Subvastus Approach Supporting Fast-Track Total Knee Arthroplasty Over the Medial Parapatellar Approach: A Systematic Review and Network Meta-Analysis. Journal of Arthroplasty, 2023; 38, 2750-2758
- Roysam GS, Oakley MJ. The Subvastus Approach for Total Knee Arthroplasty Resulted in Better Short-Term Outcomes than Did the Parapatellar Approach. A prospective, randomized, and observer-blinded trial. J Arthroplasty. 2001;16:454–457. doi: 10.1054/arth.2001.22388.
- Chang CH, Chen KH, Yang RS, Liu TK. Muscle torques in total knee arthroplasty with subvastus and parapatellar approaches. Clin Orthop Relat Res. 2002;98:189–195. doi: 10.1097/00003086-200205000-00027
- Sastre S, Sanchez MD, Lozano L, Orient F, Fontg F, Nun˜ez M. Total knee arthroplasty: better short-term results after subvastus Approach. A Randomized, controlled study Knee. Surg Sports Traumatol Arthrosc. 2009;17:1184–1188. doi: 10.1007/s00167-009-0780-6.